

















 30 / 72
30 / 72

fracture healing in osteoporotic bone have also been conducted
based on the diaphyseal model of Bonnarens and Einhorn with an
obvious gap between experimental surgical methods in midshaft
long bones that is somewhat deviated from the clinical relevance of
metaphyseal fracture in patients [13,77
–
84]. Therefore, the conclu-
sions of these studies are limited and more clinically relevant animal
model focused on the metaphyseal bone area would make our
understanding on fracture healing in osteoporotic bone more
comprehensive.
Small animal models for metaphyseal fracture healing in osteopor-
osis must meet three general criteria. First, the metaphyseal region of a
long bone is targeted and a complete discontinuity of this area is
accomplished by osteotomy or other means. Second, the type of
internal fixation should mimic as good as possible the clinical situation
which means that mainly plate fixation techniques should also be used
in animals. The third criterion is by far the most difficult one to achieve,
which is an osteoporotic or at least osteopenic bone status in small
animals comparable to the human situation. This bone mineral density
reduction procedure should be carried out reflecting the underlying
study aim focusing either on type 1 (post-menopausal) osteoporosis,
primary type 2 (senile) osteoporosis or secondary osteoporosis.
Possible ways of induction of osteoporosis with all pros and cons
have recently been reviewed by Simpson and Murray et al. (2015) in
this context [85].
The first model that mimicked those clinical properties on targeting
metaphyseal fractures with plate fixation in small animals was
introduced by Stürmer et al. (2010) in a study that was primarily
dedicated on the effects of estrogen and raloxifene in the early phase of
fracture healing in osteoporotic bone [86]. Surgical technique included
an anterior
–
medial approach from the medial femur condyle to the
middle of the tibia. A transverse osteotomy of the proximal tibia
metaphysis was performed followed by plate fixation of the proximal
tibia with a T-shaped titanium plate. As the animals underwent
ovariectomy during the osteotomy procedure, osteoporotic bone status
cannot be claimed for this series.
Alt
’
s group recently published a rat model on the metaphyseal area
of the distal femur with different gap sizes to mimic fracture defect
healing in ovariectomized rats for the potential use of biomaterials to
stimulate fracture healing [87]. In contract to the model Stürmer et al.,
the rats were ovariectomized 12 weeks before osteotomy leading to a
significant reduction in bone mineral density compared to sham-
operated animals at the time of distal femoral osteotomy. Furthermore,
the distal femur was used allowing for a greater defect region
compared with the proximal tibia metaphysis. The third difference
was the wedge-shaped osteotomy in the femur with a lateral height of
3 or 5 mm in relation to the horizontal osteotomy without significant
defect on the proximal tibia by Stürmer et al. This study showed that
wedge shaped fracture defects with a lateral height of 3 mm was
leading to stable bone healing after 6 weeks whereas 5 mm defects did
not consolidate and can therefore be considered as a critical size
fracture defect model.
As mentioned above, the study of Stürmer et al. [86] used
ovariectomy at the time of osteotomy and phytoestrogen-free pelleted
food for the duration of the study of 35 days which limits the effects of
bone mineral density reduction to 35 days. The study design contained
four different treatment groups: osteopenic control with ovariectomy
(OVX) (group I), sham-operated animals without ovariectomy (group
II), osteopenic animals with ovariectomy treated with estradiol
benzoate (group III) and osteopenic animals with ovariectomy
treated with raloxifene (group 4). After 35 days, all osteotomies had
healed in all groups but the OVX group exhibited a significantly lower
yield point compared to the sham animals in biomechanical testing.
Regarding treatment effects, estrogen and raloxifene improved the
biomechanical properties of bone healing compared to OVX with a
denser trabecular network for estrogen treatment. Raloxifene greatly
induced total callus formation in contrast to estrogen which mainly
enhanced new endosteal bone formation.
Alt et al. performed a study on the comparison of fracture defect
healing in 3 mmwedge shaped defects based on the above mentioned
animal model between ovariectomized and non-ovariectomized rats in
which both groups received a calcium-, phosphorus- and vitamin D3-,
soy- and phytoestrogen-free diet [87,88]. After the evaluation period of
6 weeks, one of the two non-destructive three-point bending tests
with at 3 mm lever span showed a significant reduction in the lower
flexural rigidity in the OVX group compared to the sham group.
However, the 10 mm lever test did not yield a statistical significant
difference. This might be related to the fact that the bending test at
3 mm distance to the femoral condyles mimics more a shear test
arrangement due to the close application of the load to the healing
zone. The 10 mm test can be rather considered as a real bending test
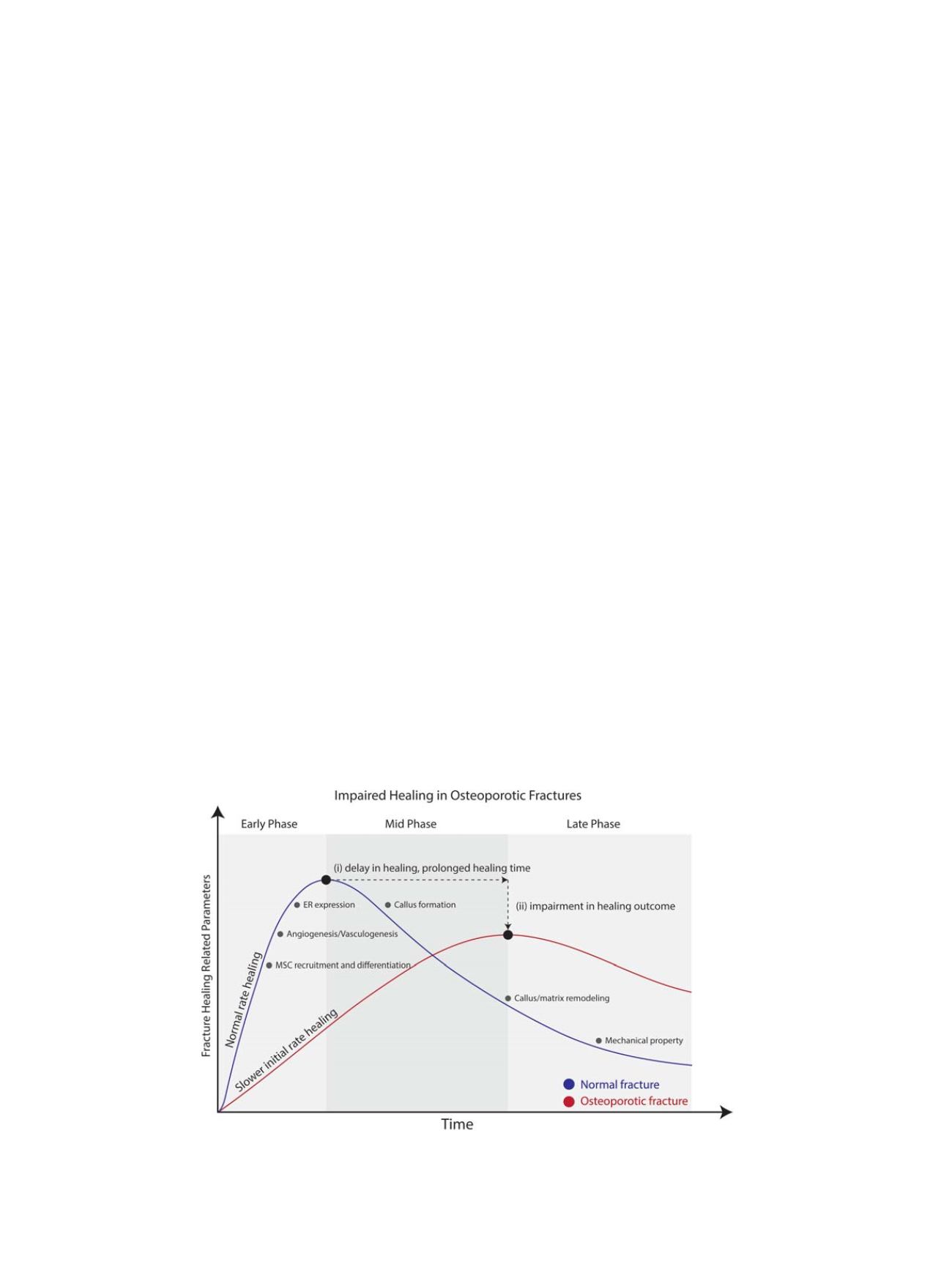
Fig. 1.
Impairments in Osteoporotic fracture. Osteoporotic fracture healing often demonstrates (i) delayed healing and (ii) impairment in healing outcome. Factors that were
observed to be impaired include MSC recruitment and differentiation, angiogenesis, vasculogenesis, and ER expression during the early phase of fracture healing. Callus forma-
tion capacity and the subsequent callus/matrix remodeling was also shown to be impaired during the mid to late phase of osteoporotic fracture healing. These impairments
would ultimately determine the healing outcome in mechanical property of the healed bone.
W. H. Cheung et al. / Injury, Int. J. Care Injured 47S2 (2016) S21
–
S26
S24