

















 36 / 72
36 / 72

could be performed at many medical care centers without much
additional work.
Distal radius fractures
Distal radius fractures in the elderly population have a second
incidence peak [30] and, consequently, represent a frequent form of
osteoporotic fracture after low energy trauma. Regardless of bone
quality, surgical management of distal radius fractures has undergone
extensive changes over the last four decades, progressing from casting,
to K-wire fixation followed by dorsal plating and finally palmar locked
plate fixation. According to current biomechanical studies the latter
offers very good primary stability [31]. In the clinical setting, palmar
plate fixation has also produced very good results in terms of stability
and minimization of reduction loss [30] even in multifragmentary
osteoporotic situations [32]. Based on our clinical experience and
scientific analyses [30] there are virtually no restrictions as far as bone
quality is concerned on the application of locking implants in the
surgical management of distal radius fractures. The implantation of
bone substitute materials, e.g. calcium phosphate, to augment the
dorsal defect zone, for which there is no verifiable evidence [33], has
become more or less obsolete with the advent of
“
modern
”
implants
[34]. Nonetheless, if preoperative diagnostics and surgical planning
identify contraindications to plate fixation, e.g. extensive comminution
of the epiphysis and/or extremely distal fracture morphology, then
transfixation of the joint is a very good alternative in terms of both
reduction loss and long-term function of the wrist [35]. Since the
fixation pins are inserted into the cortex, stability is less affected by
osteoporosis. Given the good outcomes achieved with these two
treatment methods it is still noteworthy that current studies report
comparable or sometimes even better functional outcomes for
conservative treatment compared with surgical joint reconstruction
in the geriatric population [32,36]. These findings should be carefully
considered when selecting the therapy regimen since they help to put
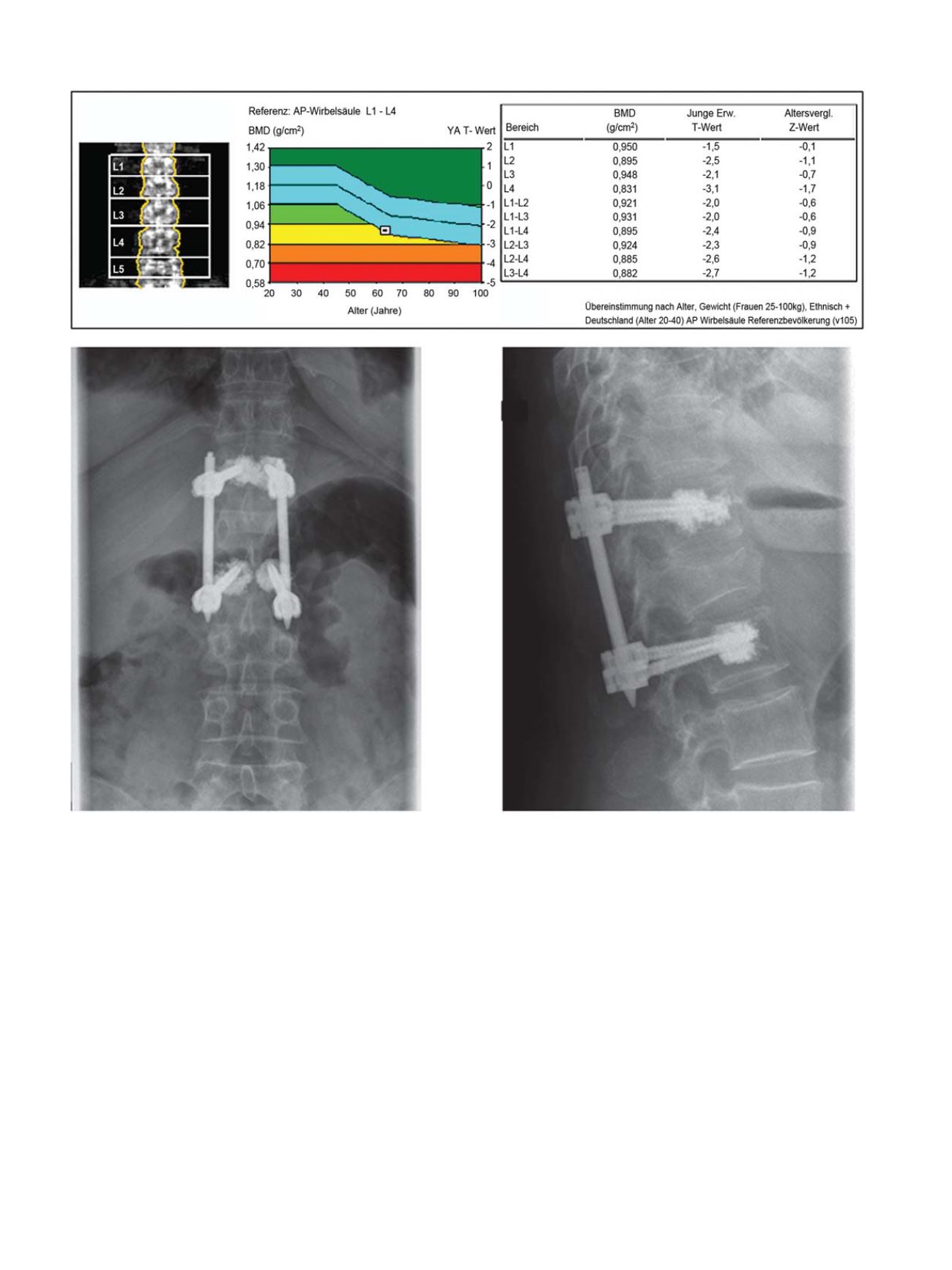
Fig. 3.
Treatment algorithm in the presence of osteoporosis. In this 64-year old female patient we decided that her painful, progressive kyphosis was an indication for closed
reduction and minimally invasive dorsal stabilization. Given the osteoporosis values from DXA testing and based on our hospital
’
s in-house algorithm we decided on PMMA
augmentation of the pedicle screws.
L. Konstantinidis et al. / Injury, Int. J. Care Injured 47S2 (2016) S27
–
S32
S30