

















 35 / 72
35 / 72

cornerstone of surgical management and has a tolerable early
complication rate [17]. Furthermore, there is an option to perform a
four-segment bridging as an extension of dorsal instrumentation
towards the cranial and caudal aspects by one segment. Cement
augmentation of pedicle screws or even simultaneous kyphoplasty of
the affected vertebrae are ways to support the ventral column and
potentially preempt failure. Existing literature however does not reveal
sufficient clinical data to answer the question of when the afore-
mentioned adjuvant measures are indicated nor to solve the dilemma
of which technical option will provide better protection from
mechanical failure or the development of adjacent fractures [16]
(Figure 2). The decision can only be based on subjective criteria and is
dictated more by eminence and less by evidence-based criteria. The
relevant literature provides certain hints for a correlation of BMD with
mechanical stability related to screw anchorage. The standard work on
this matter is that of Wittenberg et al. [18], which correlates pedicle
screw fixation with bone density (QCT) in the experimental setting. A
threshold value of 90 mg/cm
3
has been identified as a good predictor
for failure. In a more recent study by Paxinos et al. [19] a BMD of
150 mg/cm
3
has been identified as the threshold value below which
mechanical stability of dorsal instrumentation was reduced. This value
was however based on in-vitro data, whereby it is close enough to the
findings of Wittenberg et al for these data to be regarded as valid
reference values. Furthermore, the literature offers numerous biomech-
anical analyses that correlate the fixation stability of vertebral
derotation spondylodesis (VDS) with bone quality based on DXA or
QCT. As might be expected the findings reveal a correlation between
BMD and mechanical stability in pull-out testing, but a threshold value
to indicate failure risk was not defined [20]. One of the biomechanical
studies conducted at our institute [21] compared ventral cage
spondylodesis with and without dorsal instrumentation. The study
confirmed the assumption of higher stability for the combined
procedure and also identified a BMD cut-off value below which the
stability of isolated ventral stabilization is at risk. The value obtained
from this studywas 220 mg/cm
3
, which is at about the same level as the
threshold value identified for proximal femur fractures.
These values have been cited in a number of publications, but
have not yet been introduced for application in clinical practice. The
reasons for this might be that, as for proximal femur fractures, QCT is
not possible at the pre-operative stage at most institutions. Even the
suggestion of evaluating these values in the clinical setting, which is
not happening at this time, may be considered by clinicians with
scepticism.
At our institution we perform DXA for vertebral body fractures if
the patient is in an age group typically susceptible to osteoporosis. If
the indication for surgical stabilization is given, we favor minimally
invasive, bisegmental, fourfold dorsal instrumentation with PMMA
augmentation of all four pedicle screws for a T-value less than
−
2.0 SD
(Figure 3). So far, we have been able to clearly reduce the risk of failure
with this procedure. Nevertheless, this value is based on purely
subjective criteria and clinical experience, whereby it does embrace
the threshold stated in the national recommendations for medicinal
therapy for osteoporosis [22].
Proximal humerus fractures
Proximal humerus fractures are another large group of injuries
typical for osteoporosis. In many cases non-surgical management
is possible and achieves acceptable or even very good functional
outcomes [23,24]. However, in cases of severe dislocation or in unstable
fractures surgical intervention must be considered [23]. The compet-
ing options today are locking screw plate fixation or intramedullary
nailing. If the articular cartilage ( joint) has extensive damage, joint
replacement becomes an option to consider either as an anatomical
joint prosthesis or as a reverse prosthesis [23]. Unfortunately, clearly
defined decision-making criteria relevant to surgical, non-surgical
treatment or even joint replacement have not yet universally agreed. In
reality, current management of these fractures is dictated more by
institutional circumstances and subjective criteria [23]. Although
evidence-based research is sparse [25] this section addresses the
search for threshold values relevant to osteosynthesis of proximal
humerus fractures by plating or nailing. As for the proximal femur,
early fixation failure in humerus fractures is manifested as screw cut
out from the cancellous bone at the articular surface with consequent
tilting of the cortex, generally into varus, and resultant fracture
dislocation (Figure 4). Delayed failure in the form of humeral head
necrosis is a different entity because it derives from fracture-related
compromise of cortical vascularity. Early failure rates can be as high as
20% [26]. The quality of the fixation depends not only on the suitability
of the implant and correct axial alignment of the reduction, but also on
screw anchorage in the cortical bone. In contrast to the femoral head,
the cancellous structure of the humeral head shows large local
variations. At the periphery subchondral bone can be found which is
very dense [27,28], and it is in this area that the implants should be
anchored even though it is associated with the risk of intraarticular
screw penetration. The central region of the humeral head may contain
very little bone and provides almost no mechanical support for the
anchorage of metallic implants. Due to this inhomogeneous nature of
the trabecular bone in the humeral head it is difficult to interpret an
overall BMD measurement.
Numerous biomechanical studies have compared different osteo-
synthesis procedures in cadaveric bones. The majority of studies
found a strong correlation between failure and BMD, but since these
series were comprised of approximately 6
–
8 pairs of bones only, it is
not possible to determine a BMD cut-off value to predict failure.
Fortunately, data from a prospective clinical study that investigated
various parameters which were then compared with failure after
surgical management of proximal humerus fractures are found in the
literature [26]. As expected bone density expressed as BMD calculated
from CT images strongly correlates with failure. The authors even
state a BMD value of 95 mg/cm
3
as a threshold value below which
the risk of failure rises markedly, whereby the precise algorithm for
BMD computation from CT data is not expanded in detail in that
publication. However, the same team has published a well designed
and established method of calculating BMD from CT data for the
contralateral limb [29]. The fact that the data cited above are based
on a clinical study increases the statement validity of the values,
making it easier to transfer theory into clinical practice. In addition,
preoperative CT diagnostics for proximal humerus fractures are part
of standard procedures in many institutions, which means that
even the preoperative analysis of the predictive factor
“
osteoporosis
”
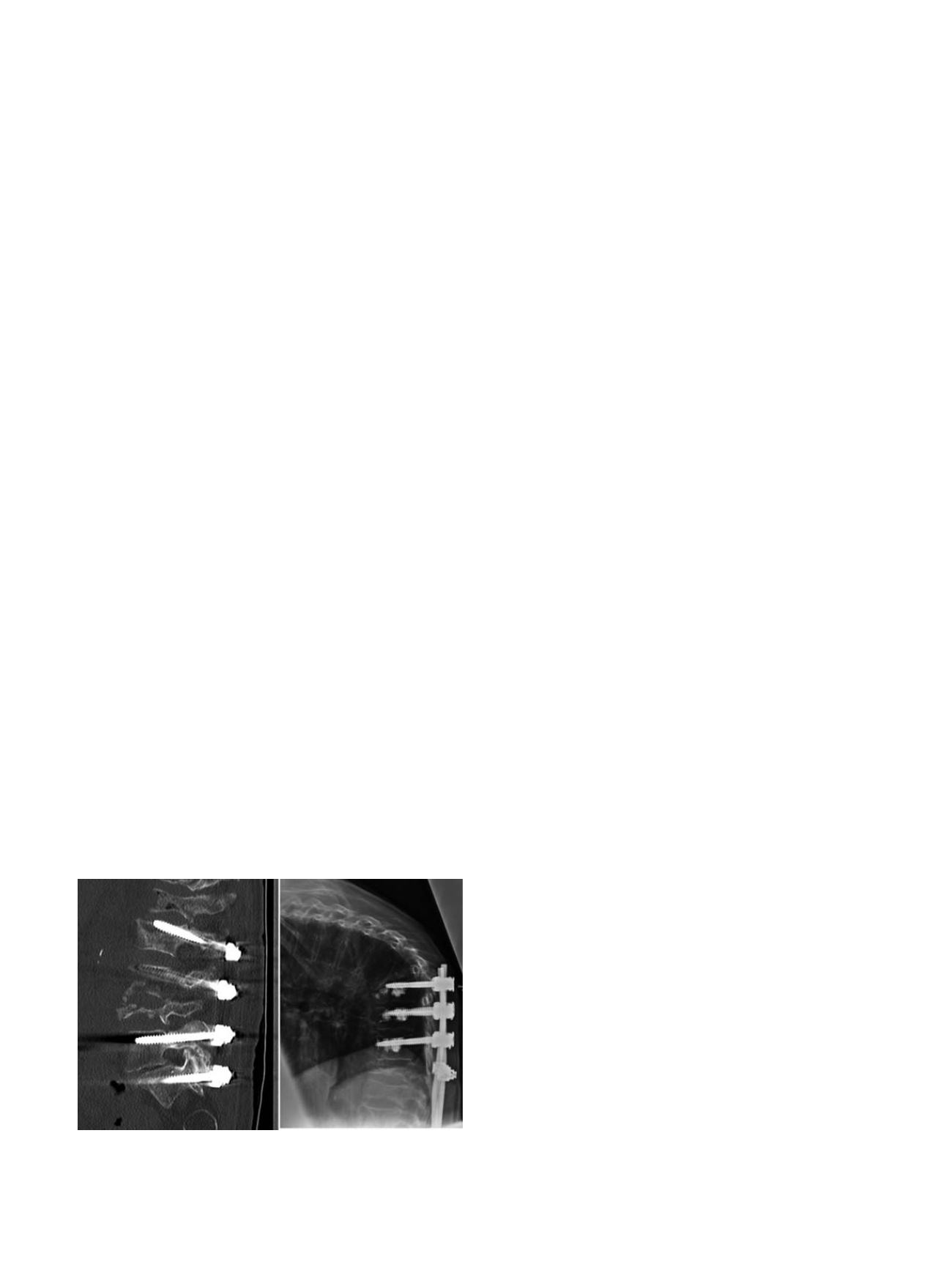
Fig. 2.
Sectional CT imaging after surgical intervention for osteoporotic subsidence
fractures. On the left side cut out of the cranial screws occurred despite the four
segment bridging. On the right side another complication typical of extensive fusion
is illustrated, namely, fracture of the adjacent cranial vertebral body.
L. Konstantinidis et al. / Injury, Int. J. Care Injured 47S2 (2016) S27
–
S32
S29