

















 44 / 72
44 / 72

screws in combination with angular stable plates enable fracture
fixation in a conventional way and allow in-situ augmentation of the
screws with polymethyl-methacrylate (PMMA) cement (Figure 1b).
In a biomechanical in-vitro study, the effect of in-situ augmentation
on implant anchorage was investigated in a three part fracture model
[23]. Fracture fixation was carried out using an angularly stable plate
and cannulated screws to allow for the augmentation of the proximal
screws with 0.5 ml of PMMA cement. Paired humeri (control and
augmented) with reduced bone quality were used for two differently
simulated loads (torsion and varus bending). Cyclic loading, with a
constantly increasing load magnitude, to implant fixation failure was
applied in both loading conditions. Compared to the contralateral
control group, augmentation resulted in a significantly increased
number of load cycles and failure for varus bending and torsional
loading. While implant anchorage showed a strong correlation with
bone quality in the control group, the augmented group showed no
correlation between implant anchorage and bone quality. However, it
was shown that the improvement of implant anchorage by augmen-
tation (difference between control and augmentation) correlated with
bone quality, and augmentation was most effective in low bone quality
and negligibly effective in good bone quality (Figure 2).
Due to a non-uniform distribution of bone quality in the humeral
head, investigators still debate which and how many screws are most
beneficial for augmentation. In order to determine which screws had
the least purchase and would benefit the most from augmentation, a
study was performed evaluating the local bone quality in the humeral
head by measuring the breakaway torque at the screw tip [24]. The
screws in the anteromedial and anteroinferior aspects of the humeral
head showed the lowest breakaway torques and were selected for
augmentation with 0.5 ml of PMMA cement. Using a similar test setup
for varus bending, the effect of in-situ augmentation of two screws
with the lowest breakaway torque achieved almost the same stability
as augmentation of the four most proximal screws.
Augmentation techniques for hip fractures
According to epidemiologic data, there is an increasing incidence of
hip fractures, with an estimated 1.7 million fractures worldwide per
year in 1990 to an expected number of 6.3 million per year in 2050 [25].
Given the importance of maintaining function and independence in
the geriatric patient population, the use of PMMA for augmentation of
fixation in hip fractures is of growing. The use of bone cement
augmentation has been reported for plate, screw, and nail osteosynth-
esis in elderly patients [26,27], demonstrating increased bone-implant
interface, improved implant anchorage, reduced screw cut-out, and
improved early full-weight bearing [26,28]. The treatment of trochan-
teric fractures with a DHS (Dynamic Hip Screw) augmented with
PMMA or a resorbable bone cement based on calcium phosphate has
shown greater biomechanical strength, faster pain reduction, and
improved healing compared to a control group [27].
In a clinical prospective study of 64 patients with 31-A2 and 31-A3
fractures of the proximal femur, treatment with a PMMA-augmented
DHS showed good fracture consolidation without any adverse
complications such as avascular necrosis of the femoral head [29].
However, intramedullary nailing was associated with improved
biomechanical stability relative to extramedullary fixation techniques
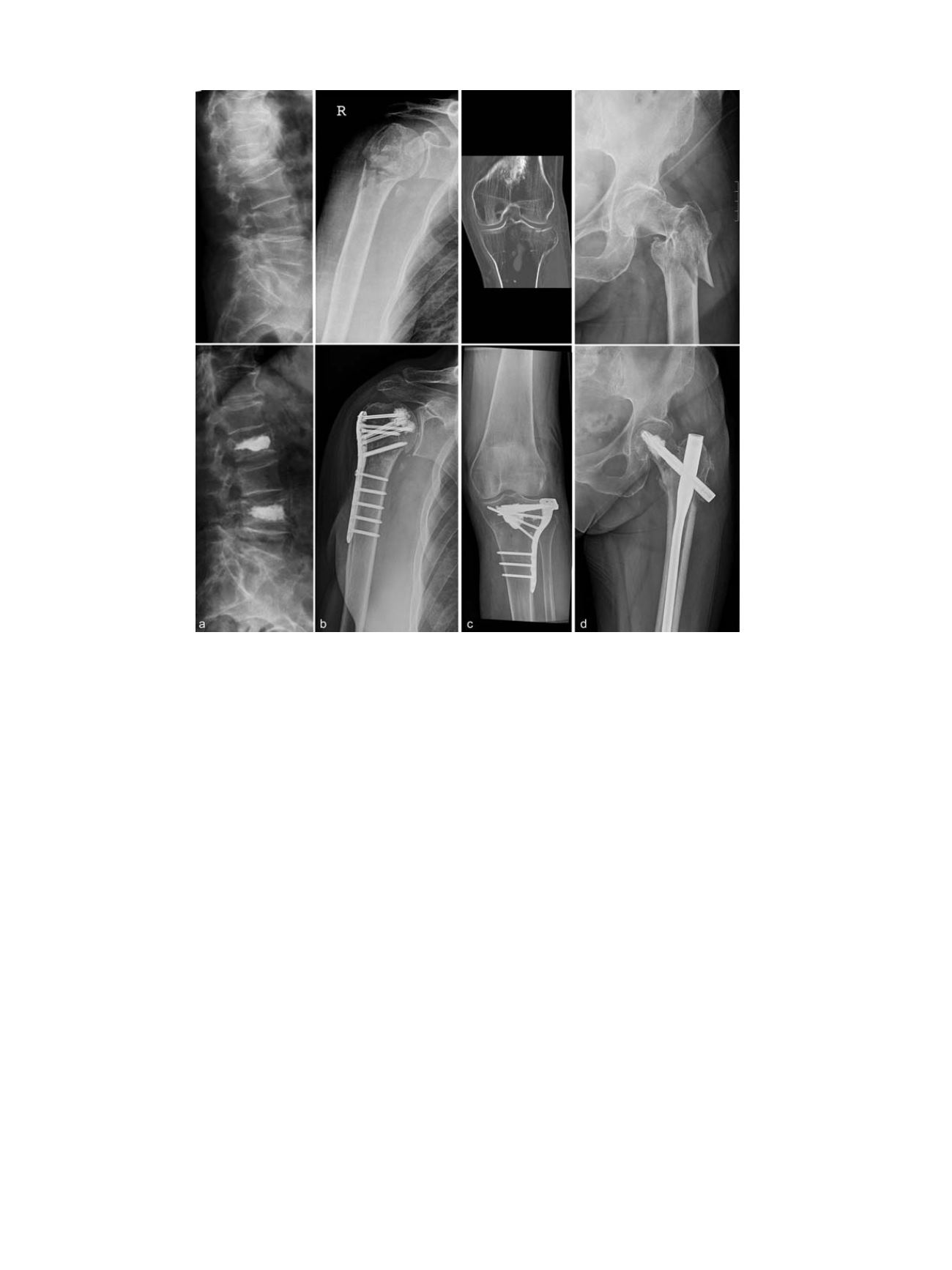
Fig. 1.
Pre- and post-operative radiographs after operative treatment using different augmentation techniques. (a) vertebral fracture treated with PMMA kyphoplasty; (b) prox-
imal humerus fracture treated with a PMMA augmented plate osteosynthesis (PHILOS ®); (c) proximal tibia fracture treated with internal fixation after filling of the subchondral
void with calcium-phosphate cement; (d) trochanteric fracture treated with a PMMA augmented PFNA (Proximal Femur Nail Antirotation, Fa. Synthes).
C. Kammerlander et al. / Injury, Int. J. Care Injured 47S2 (2016) S36
–
S43
S38