

















 45 / 72
45 / 72

[26], and the use of PMMA-augmented intramedullary nailing of
proximal femur fractures is another potential area for improved
fixation using augmentation techniques. Using a special high viscosity
bone cement (Traumacem V+) applied via a PFNA blade, augmen-
tation can be safely and effectively achieved using similar standard
implantation techniques to the non-augmented device [28]. Instead of
the conventional spiral blade (Figure 1d), a perforated spiral blade is
used in cement-augmented PFNA nailing to better achieve dissemin-
ation of the cement in the femoral head. Prior to the introduction of
cement using this technique, the possibility of intraarticular leakage
into the hip joint should be evaluated by injecting a dissolved contrast
agent, which can subsequently be cleared with a saline flush. After
mixing a high viscosity bone cement (such as Traumacem V+) with a
specially-designed cement kit, the bone cement is injected into the
blade by using a trauma needle kit under fluoroscopic control.
Approximately 3
–
5 ml of cement should be injected via the blade,
not to exceed a maximum volume of 6 ml bone cement should not be
exceeded. Hardening of the cement takes about 10
–
15 minutes [30]. In
the intra- and post-operative radiographs, a central distribution of
bone cement around the top of the spiral blade is desirable.
Augmentation techniques for tibia plateau fractures
Tibial plateau fractures make up about 2% of all fractures and about
10% of fractures in the elderly. This type of fracture usually results from
direct axial compressive forces applied in conjunction with a valgus
force. With increasing age, the subchondral bone and the underlying
cancellous bone are less able to resist axial loading, resulting in a split
or depressed fracture. The treatment goal, as with most intraarticular
fractures, is to reestablish joint congruency, and restore range of
motion, alignment, and stability. One of the major problems with
fractures that involve a depressed articular fragment is to maintain the
reduction of the fragment during the course of healing.
The classic method to support the elevated articular fragment is
through filling of the subchondral voidwith autologous or allogenic bone
transplant. However, conventional bone transplants are often weak, and
weight-bearing during healing has to be restricted to prevent subsequent
displacement of the fracture and avoid subsidence of the elevated articu-
lar fragment; full weight-bearing is usually restricted for 6
–
12 weeks
post-operatively, includingwhenbonegraft is used [31
–
33]. Inaddition to
the lackof adequatemechanical support during healing, autologous bone
transplants are also associated with draw-backs related to donor-site
morbidity that can be significant. As a substitute to autologous bone
transplants, various biomaterials have been introduced for use in the
filling of subchondral voids in tibial plateau fractures (Figure 1c).
Composites for subchondral void filling offer a variety of potential
options with regards to their physical, mechanical, and biological
properties. These materials frequently are available as preformed
blocks that can be tailored to defects as well as substances that are
injectable and self-hardening materials to fill bone voids intraopera-
tively. The mechanical property most often used to characterise the
mechanical behavior of a bone graft substitute is compressive strength,
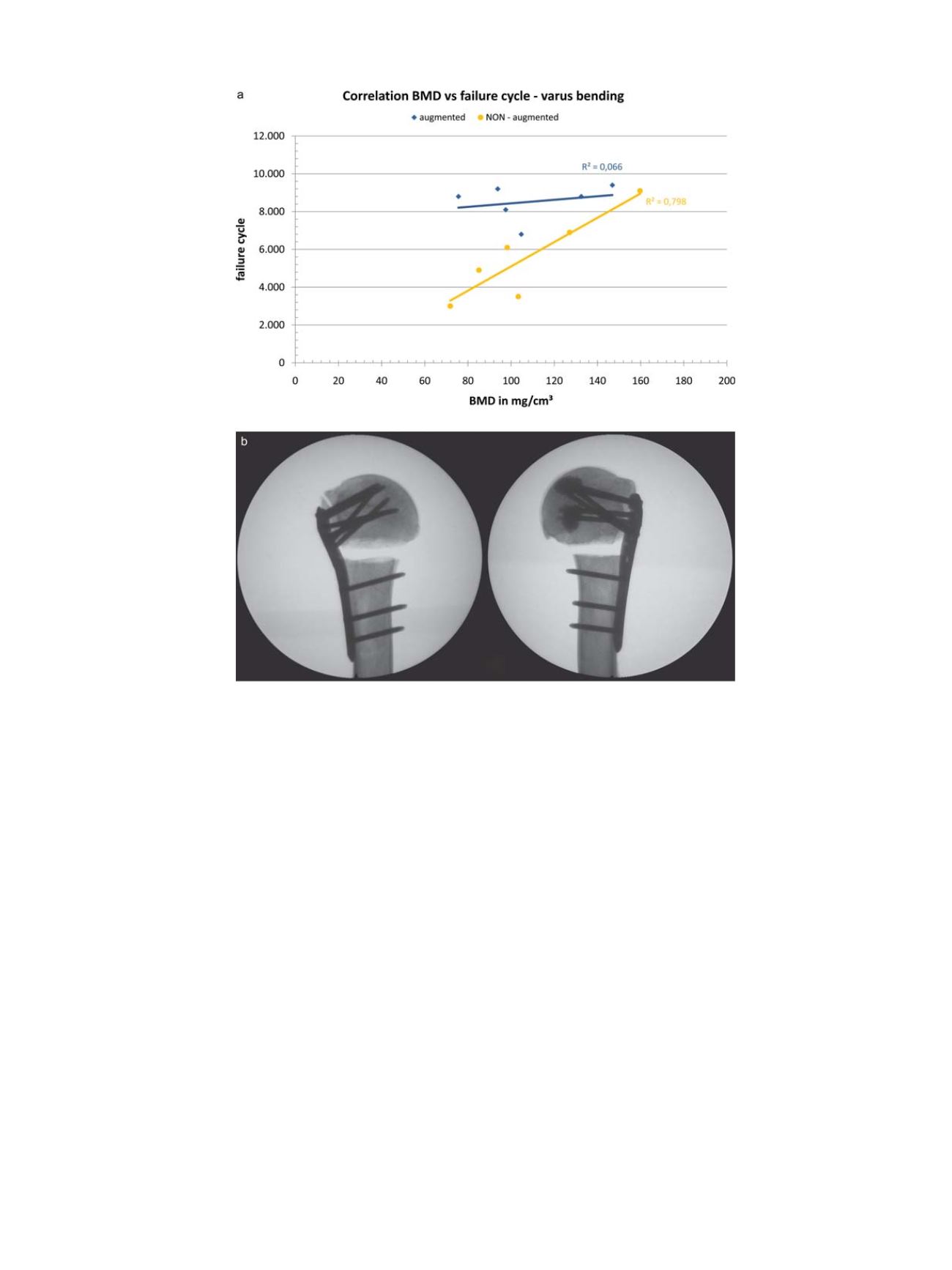
Fig. 2.
Biomechanical analysis of cement augmented plate osteosynthesis in a proximal humerus fracture. (a) Graphic representation of the correlation of BMD vs. failure cycle
and (b) Radiographic image of the model used for the mechanical testing [23].
C. Kammerlander et al. / Injury, Int. J. Care Injured 47S2 (2016) S36
–
S43
S39