

















 40 / 72
40 / 72

Modern locked plating technology was introduced in the 1990
’
s,
in part to address the difficulties with treatment of osteoporotic
metaphyseal fractures [7]. Locked plates allow the screw heads to
thread into the plates, creating constructs that are
“
fixed-angle,
”
which
is theoretically better able to resist varus displacement of the fracture
(Figure 2) [8]. These implants have provided an excellent tool to
achieve stable fixation in many osteoporotic fractures [9,10].
Limitations of locked plating
Although the mechanical basis for locked plating seems ideally
suited for the osteoporotic metaphyseal fracture, it has not turned out
to be the panacea that was originally hoped. Most surgeons have
transitioned to using locked plates for these fractures based on
anecdotal observations of patient outcomes, but there is a paucity of
clear, high-level evidence proving their benefit [11]. In addition, there
are other limitations related to locked plating in this application. Even
through the screw heads mechanically lock to the plate, in order for the
fixation to remain stable, the screw shafts must remain securely
anchored in the epiphyseal, periarticular bone segment [11]. For this to
occur, there needs to be an adequate volume of bone with adequate
quality to provide anchorage. Fractures that occur very distal,
particularly in supracondylar femur fractures adjacent to a total knee
arthroplasty, may have limited native bone stock available for placing
effective locking screws. Additionally, severe osteoporosis,
e.g.
with
trabeculae that are not visualized on CT scan and appear as a void,
often precludes stable implant fixation. In these difficult situations,
consideration can be given to augmenting the metaphyseal region
with exogenous material such as
“
cement
”
bone void fillers to provide a
mechanical substrate so the locked screws function as
“
rebar
”
to
maintain fixation [12]. Commonly used augmentation material
includes biological cements, such as calcium phosphate (Figure 3),
fibular allografts (Figure 4), or polymethylmethacrylate (PMMA) [13].
Intramedullary nailing
Intramedullary nails have also evolved lately so that fracture
fixation with a nail is more predictable than in the past. Similar to
locked plates, intramedullary nails that are longer, have more screw
options for fixing short osteoporotic segments, as well as fixed
–
angled
capabilities are now available for treating difficult fractures such as
those described here [14]. We have found in our practices that modern
nails are quite effective for most of the fractures that are commonly
treated with anatomically-contoured locked plates, the exceptions
being comminuted articular fractures, those with one
very
short
periarticular segment, or those with arthroplasty components that
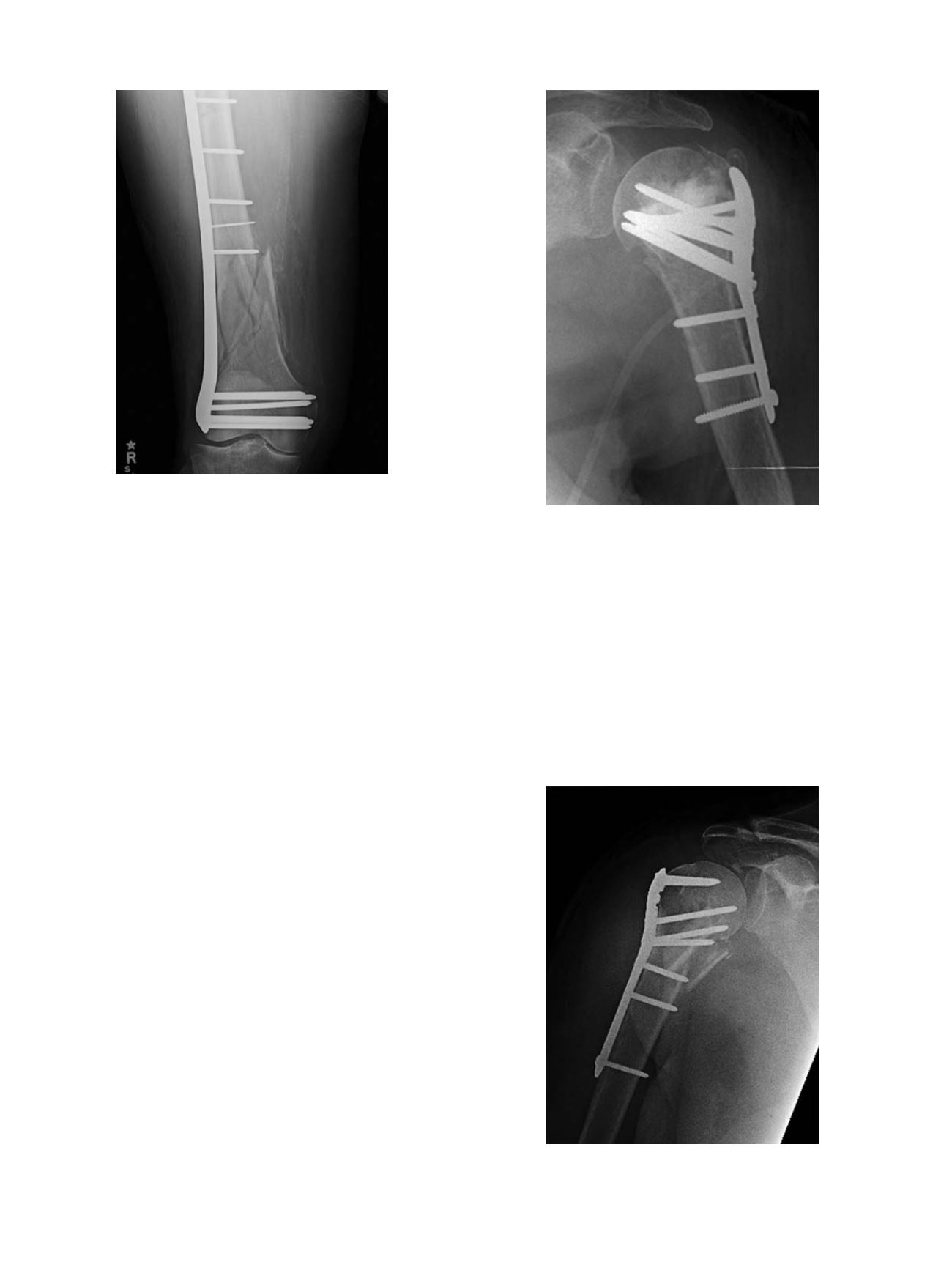
Fig. 2.
Example of successful bridge plating of a comminuted metaphyseal
supracondylar femur fracture in an elderly patient.
Fig. 3.
One option for augmenting fixation in osteoporotic proximal humerus frac-
tures is calcium phosphate application to fill the metaphyseal void and provide
increased substrate for locked screw purchase.
Fig. 4.
Another option for augmentation in proximal humerus fractures includes use
of a fibular strut allograft, which in this case functions as a medial cortical substitute
to enhance overall construct stability [16].
C. Collinge, M. J. Gardner / Injury, Int. J. Care Injured 47S2 (2016) S33
–
S35
S34