

















 58 / 72
58 / 72

fracture [9
–
12]. In clinical reality, these fracture patterns are rarely seen
and it remains unclear if these short fracture patterns accurately
represent the clinical situation or not.
Periprosthetic fracture fixation aims for the restoration of limb
function with successful bone healing and immediate load bear-
ing capacity [3,13]. The best technique for achieving this goal is
still discussed controversially. Plate fixation [5,14
–
19], cerclages
[6,11,13,19
–
24], a combination of a non-locking plate with an allograft
strut [12,20,25
–
26] and even external fixation have been described
[27]. Moreover, the technique for fracture fixation depends onwhether
the periprosthetic fracture occurred around a cemented or an
uncemented stem. Most biomechanical studies were performed with
cemented stems [6,10,11,17,28
–
31]. However, clinically periprosthetic
fractures, which show a different biomechanical performance, fre-
quently occur in non-cemented situations. Findings from early
biomechanical studies comparing strength in cemented and uncemen-
ted stems suggested a much larger load to failure for cemented stems
[32]. For the stability of osteosynthetic fixation of cemented stems,
biomechanical and clinical studies have reported that plate fixation
yields favorable outcomes when compared to either the combination
of cable fixation and a plate or just cable fixation [9,10,13,28].
To our knowledge, no biomechanical evidence exists for preferring
plate over cable fixation for typical spiral periprosthetic fractures in
uncemented stems. The first aim of our study was to assess the stability
and strength of a clinically relevant Vancouver B1 periprosthetic
fracture fixed by either a long bridging plate construct or by a cerclage
technique with titanium straps. We hypothesized that locking plate
fixation has biomechanical advantages over fixation with a simple
cerclage system. In order to achieve maximum fixation stability, we
also compared both osteosyntheses after replacing the short stemwith
a long revision stem. Thus, the second aim of our study was to assess
the mechanical difference between a fixed short stem and a fixed long
revision stem. We hypothesized that removal of the primary short stem
and revision with a long stem would show biomechanical benefit.
Materials and methods
The aim of the study was to compare locking plate fixation versus
a cerclage system and short stems versus long stems for their effec-
tiveness in managing a typical periprosthetic spiral femoral fracture.
Biomechanical testing was performed with static loading to assess
the stiffness of the fixation constructs and cyclic loading to assess
the failure strength and the cycles to failure. Twenty femur sawbones
were divided into four groups: (1) short stemwith plate fixation (
n
= 5),
(2) short stem with cerclage system (
n
= 5), (3) long stem with plate
fixation (
n
= 5), (4) long stem with cerclage system (
n
= 5).
Sample preparation
A standard femoral neck osteotomy was performed with an
oscillating saw in twenty sawbones (#3406 left femur large with
16 mm channel, 4th Generation; Malmö, Sweden). Half of the
sawbones were reamed and implanted with a cementless standard
straight short stem (AnaNova Solitär, ImplanTec, Mödling, Austria)
according to the manufacturer
’
s recommendations. The other half
of the sawbones were implanted with a cementless long revision
stem (Modular Plus, Smith and Nephew, Schwechat, Austria) after
preparing the medullary canal with a conical spiral reamer. After stem
implantation, the composite bones were potted distally into an
aluminum pot with polymethylmetacrylat (PMMA, Gößl & Pfaff,
RenCast FC 53 A/B). For proximal fixation, the prosthesis cup was
embedded with PMMA into an aluminum cylinder.
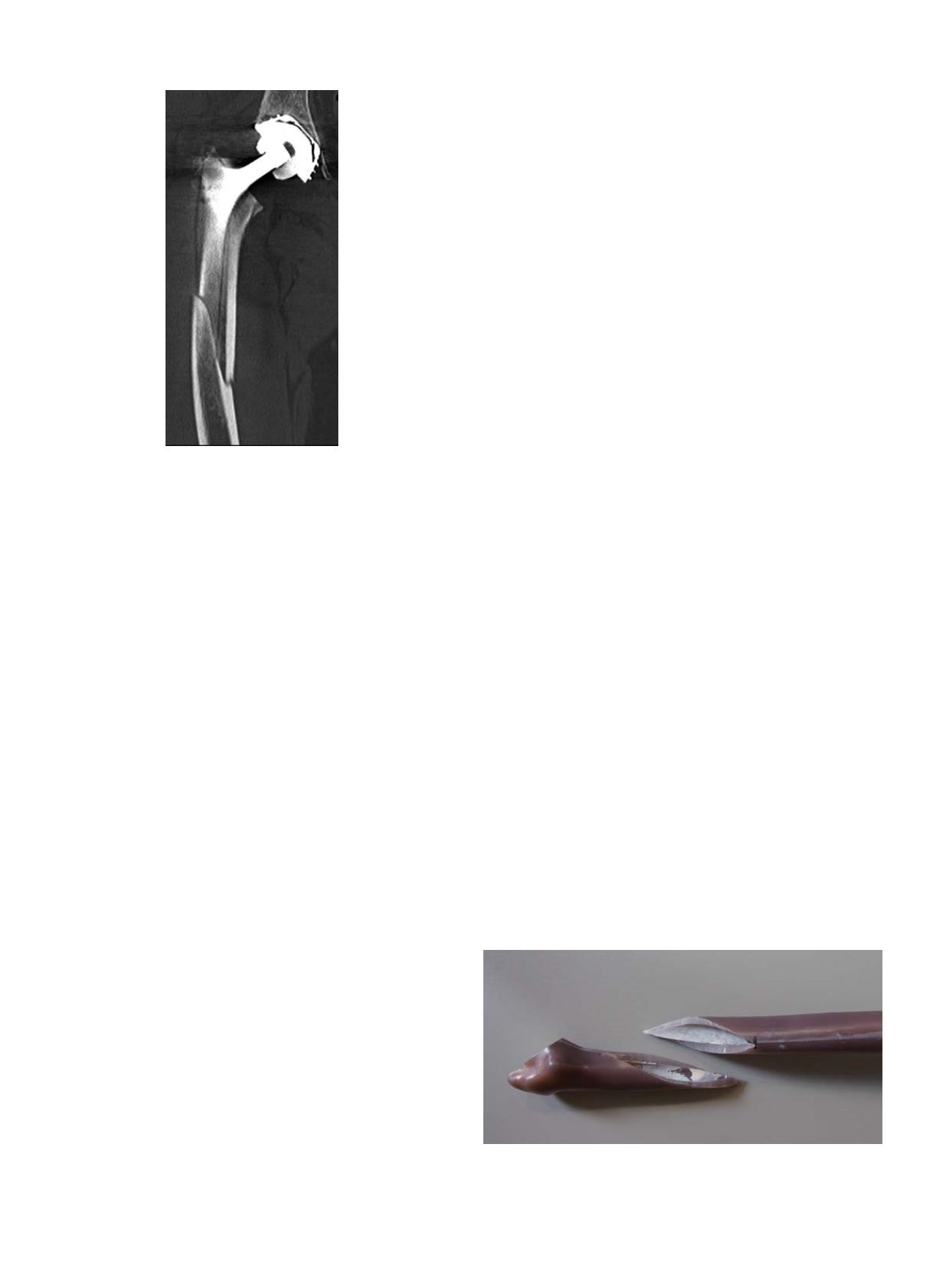
The pattern of the spiral fracture was investigated through an
analysis of CTs and plain radiographs of 30 patients with Vancouver
B1 fractures undergoing revision surgery at our institution (Figure 1).
The average length of the fracture line was 14 ± 2.2 cm and was on
average extending from 10 cm proximal to 4 cm distal of the stem. This
characteristic fracture line was drawn on the sawbones with a custom
made template. After temporary removal of the stems, the fracture line
was milled using a milling machine (Deckel FP2, Friedrich Deckel
Aktiengesellschaft, München), a rotary indexing table, and a 2 mm
diameter cutter (Figure 2).
The stems were then re-implanted into the osteotomised sawbones
with press fit stability. The proximal and distal sawbone fragments
were placed with cortical contact. The primary short stems were
carefully hammered into the sawbones. To implant the long revision
stems, which consist of two components and a multi-conical coupling
screw, the distal anchoring module was implanted first. After that,
the proximal module was implanted and secured with the screw
according to the manufacturer
’
s recommendations. In ten sawbones,
the fracture fixation was performed using a non-contact bridging
left periprosthetic proximal femur plate with 15 holes and a length of
324 mm (NCB
1
Plating System, Zimmer Biomet, Vienna, Austria).
The screw placement was performed by angulating the screws
around the implant shaft in an unlocked manner followed by locking,
utilizing locking-caps. Approximately 30° angulationwas allowed in all
directions. We placed five proximal screws (4 mm diameter cortical
screws: 1 × 50, 1 × 46, 1 × 42, 1 × 34, 1 × 32 mm) and four distal screws
(5 mm diameter cortical screws: 4 × 42 mm). Ten sawbones were
provided with the Compression Cerclage Bands (CCG
®
System,
Fig. 2.
Fourth generation sawbone model after osteotomy of the femoral neck and
creation of a standardized characteristic 14 cm spiral fracture using a template and
milling machine.
Fig. 1.
CT scan of a patient with a characteristic periprosthetic spiral type fracture,
Vancouver B1.
K. Gordon et al. / Injury, Int. J. Care Injured 47S2 (2016) S51
–
S57
S52