

















 53 / 72
53 / 72

biomechanical experiments because loosening of the stem over time
cannot be modeled adequately.
Which therapeutic possibilities do we have for interprosthetic
fractures? Numerous articles came up for periprosthetic fractures
around a hip replacement or knee prosthesis, which deal with the
various modes of treatment of these injuries. These include the
stabilization of non-stable-angle plates, angle-stable plates, cerclage
wires, additional allogeneic bone or exchange of the prosthesis
[37
–
39]. It could be shown that the stabilization with locking plates
is superior to all other methods, as long as the prostheses are not loose
[40
–
41]. If the prosthesis is loose, replacement might be the most
favorable treatment option [42]. Treatment strategies for injuries
between two implants on the femur are very limited. Apart from
specific risks that are related to the bone quality, general risk factors
such as the general condition of the often elderly patients plays also a
significant role. In addition, the particularly difficult perfusion status of
the bone increases the risk of delayed fracture healing or nonunion.
It has been shown that comparable to periprosthetic fractures in
interprosthetic fractures also some of the prosthesis are loose [43]. In
such cases, the prosthesis has to be replaced. But in these particular
cases, we have implants on the proximal and on the distal side and
under certain circumstances this can lead to a replacement of the
whole femur [44]. McLean et al. report on 5 patients with complete
exchange of the femur after periprosthetic fracture, with good results
[42]. Usually, however, plate fixation is sufficient. Mamczak et al.
describe a series of 25 patients with 26 interprosthetic fractures within
20 years that were treated with plate osteosynthesis [45]. Here, in 17
cases the distal metaphyseal part of the femur was affected while only
nine times the diaphysis below the hip prosthesis was involved. This
observation was made also by other authors, which observed most
fractures in the supracondylar region [46]. Mamczak et al. have had no
non-unions and all patients were started full weight bearing after 13
weeks [45]. The authors state that gentle surgical technique and
overlapping of the plate to the proximal and distal end of the prosthesis
to bridge the stress riser are most important. A recommendation how
far the plate should overlap the end of the prosthesis is not given. In
this context, the term
“
stress riser
”
is well known in the literature, but
precise criteria could not yet be established. Our own biomechanical
studies indicate that the distance between the implants is less
important than the cortical thickness [35]. Hou et al. report a series
of 13 patients within six years [47]. Here, in four cases, the prosthesis
on one side was loose and needs to be replaced by a longer prosthesis.
This was possible without coming into conflict with the opposite
prosthesis. All other cases were treated with locking plate osteosynth-
esis only. Unfortunately, there is no more information regarding the
localization of the fracture in this paper. The plates were so long that
they exceeded the end of the prosthesis more than twice the diameter
of the diaphysis. Important for the consolidation of fractures using a
plate osteosynthesis is the length of the implant-free zone in the femur
bone. If this is particularly short and the biological architecture is
already disturbed inmany parts of the femur, this can have a significant
effect on fracture healing. Soenen et al. Suggest, based on their
experience in a multi-center study of 14 patients that have been
classified with the Vancouver classification, to expand this classifica-
tion for these specific injuries and call these Vancouver type D fractures
[44]. In all 6 cases that were classified as Vancouver type D, after
primary care with plate osteosynthesis they noticed bone healing
disorders that needed revision either with an additional bone grafting
or complete femur replacement [44]. Platzer et al. in a series of 23
patients in 16 years also mainly used plate osteosynthesis [48]. In 4
patients with a loose prosthesis a replacement has been performed.
In 3 out of 19 cases, there was a delayed fracture healing or nonunion.
Also a very successful series of instrumentation with locking plate
osteosynthesis has been reported by Sah et al. in 22 patients over 4
years [49]. Additional cancellous bone chips were used and placed an
average of 3 cerclage in the field of hip prosthesis in 7 patients in 6
cases. The cerclage wires were used only additive in all cases. The
localization of the fractures were again mainly supracondylar.
Take together our data from biomechanical studies and clinical
reports from the literature suggest variable effects of implants to the
stability of the affected bone. Biomechanical studies have shown that a
hip prosthesis alone increases the risk for a fracture significantly. With
an ipsilateral retrograde nail the risk of fracture is double as high for the
femur, as without an implant. Therefore, extramedullary implants
seem to be superior for distal periprosthetic fractures. The situation is
different with 2 cemented prostheses on the same side [7]. Here, the
risk for a fracture is not as high as long as both prostheses are fixed. The
influence of interprosthetic distance is not as high as one might
suppose. The most important point is also not total bone density
(BMD), but the cortical thickness. These observations should be taken
into account when surgery is done at the distal end of the femur in the
presence of a hip prosthesis. If an interprosthetic fracture appeared and
there is no loosening of the stems the stabilization with locking plates
seems to be the method of choice. This could be confirmed by the data
from present clinical and biomechanical studies [9,24,44,48,49].
Augmentation as treatment option in periprosthetic distal
femur fractures
Osteoporotic fractures are an unsolved problem in today
’
s ortho-
pedic and trauma surgery [50
–
58]. Fractures of the distal femur are
associated with major complications (e.g. thrombosis, embolism,
immobilization) [50,59]. Especially the periprosthetic distal femur
fractures present surgeons with a major challenge in implant fixation
and implant anchorage. Thereby, the metaphyseal part is the most
difficult, due to the restricted space and the poor bone stock quality.
Periprosthetic distal femur fractures can be treated using different
implant options. Retrograde intramedullary nailing is only possible, if
the type of knee prosthesis allows nail insertion. Another concern of
intramedullary nailing is the methaphyseal fixation with only a few
locking bolts. This may cause secondary loss of fixation and mal-
alignment or implant loosening (Figure 4). The gold standard in the
treatment of periprosthetic distal femur fractures is the angular stable
plate fixation. But also this technique has problems in screw placement
and anchorage due to the prosthesis and poor bone quality.
In our group we investigated the implant augmentation as one
option to enhance implant fixation in distal femur fractures. In order to
improve the screw anchorage bone cement was used to increase the
load-bearing surface and thus reduce complication rate, avoiding
revision surgery, and allowing earlier mobilization of the patients.
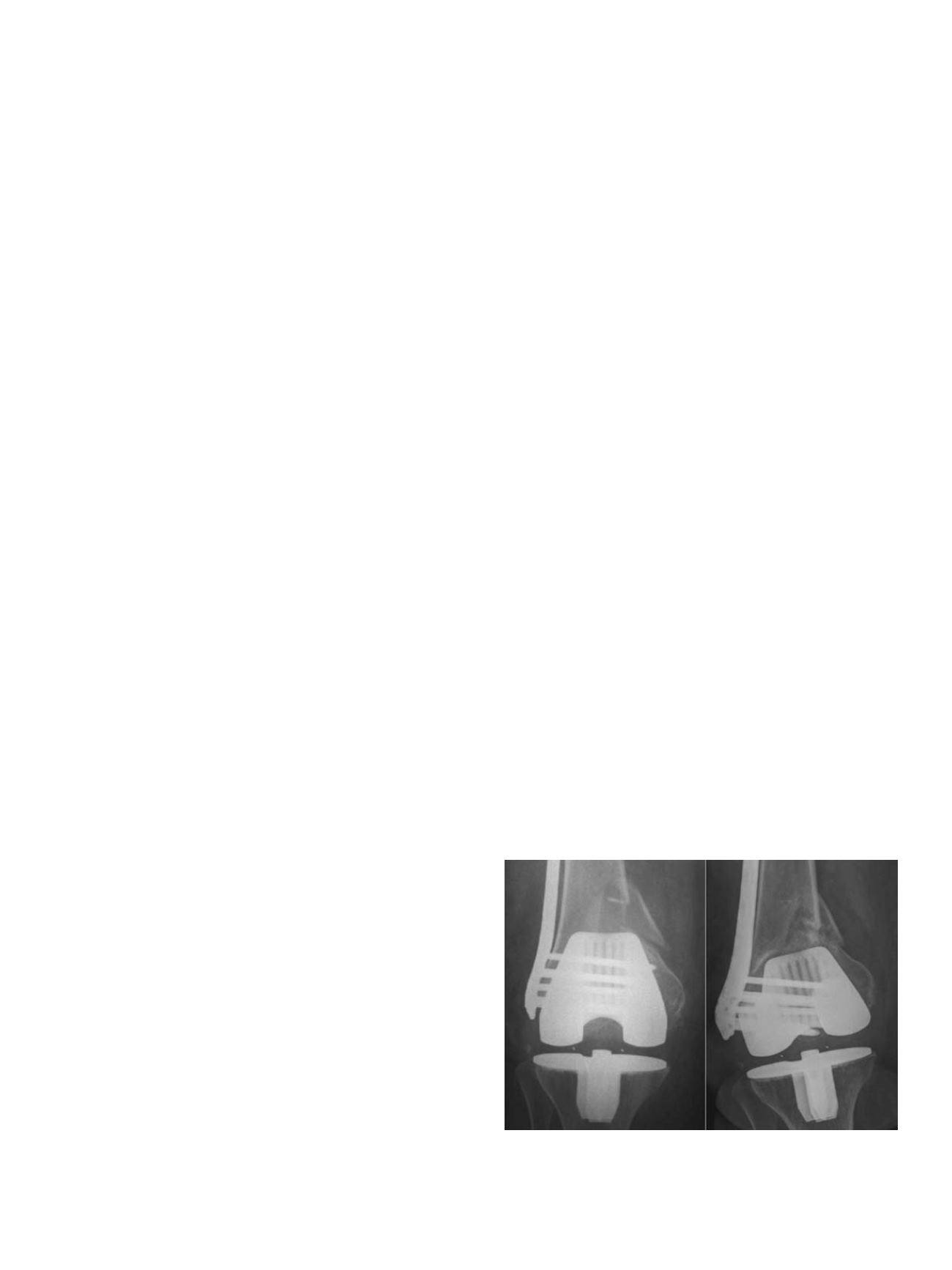
Fig. 4.
Periprosthetic distal femur fracture of an 80-year-old patient after low energy
trauma. Postoperative x-ray in ap-view after angular stable plate fixation (left) and
3-month postoperative follow-up showing the varus-failure with screw
“
cut-out
”
into the knee joint (right).
M. Lenz et al. / Injury, Int. J. Care Injured 47S2 (2016) S44
–
S50
S47