

















 55 / 72
55 / 72

In the last study on the topic of implant augmentation for the
treatment of osteoporotic distal femur fractures we used human
specimens and modified screws to establish and investigate a clinically
applicable procedure [65]. Therefore, seven pairs of fresh frozen human
distal femur specimens with low bone mass (mean age 87 years, all
female) were used. Prior to any testing bone mineral density (BMD)
was measured using QCT. In accordance with the previous studies
the LCP distal femur with an AO 33 A3 fracture model was used.
The femoral shaft has been replaced by a PMMA part and the plate was
fixed in rigid manner. In contrast to the previous studies cannulated
and perforated screws (four 1.1 mm holes in 10 and 15 mm distance
from the screw tip) were used. Thus, cement injection could be
performed after instrumentation through the screw shaft. Testing was
performed with a comparable setup; the force maximum started at
750 N andwas increased at 0.05 N per cycle. To determine failure x-rays
in antero-posterior direction were performed every 250 cycles.
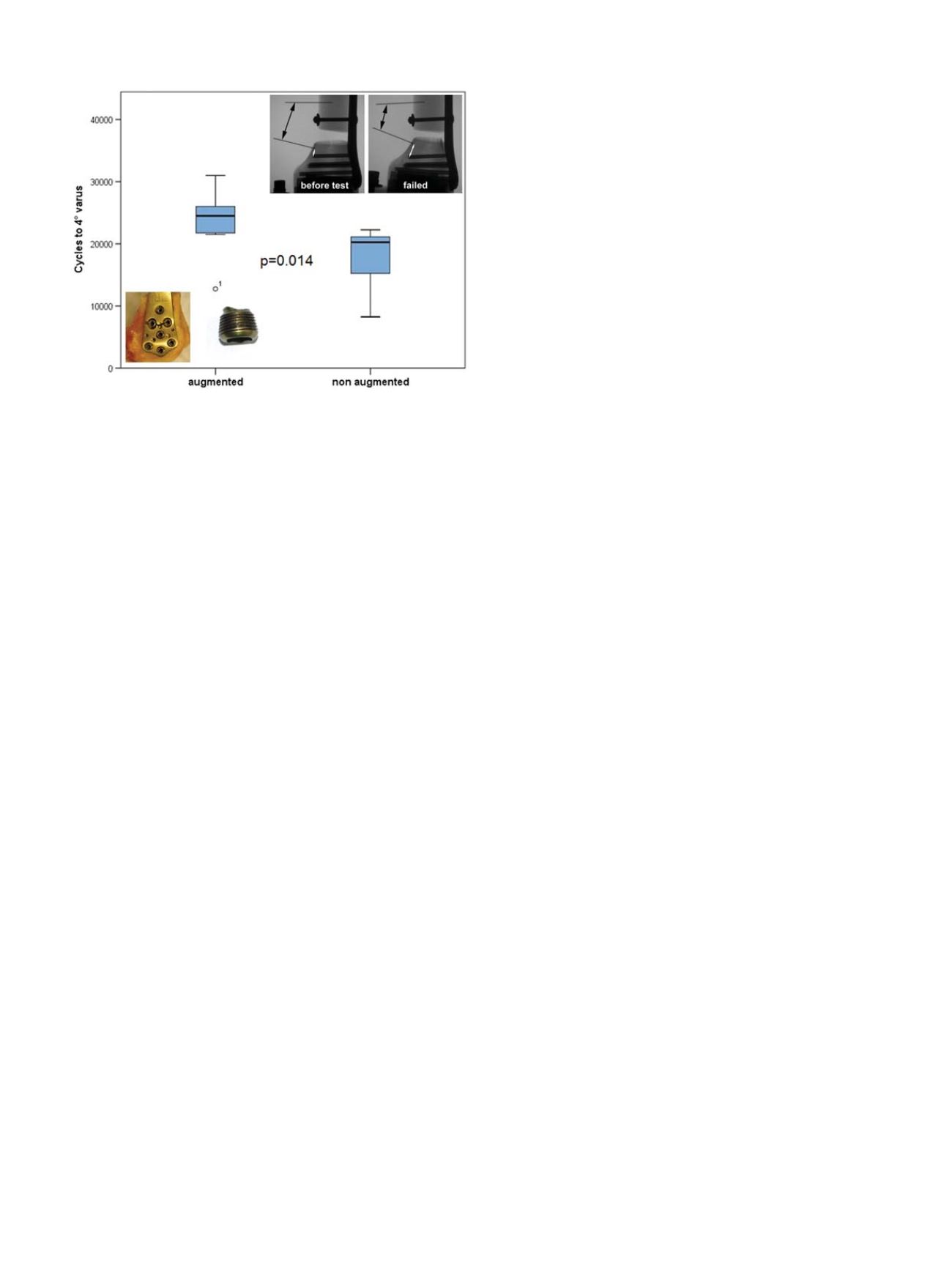
Biomechanical testing showed no significant difference for initial
axial stiffness (augmented 385.5 N/mm vs. non-augmented 366.7 N/
mm;
p
= 0.444). The mean number of cycles to failure was 23483 (SD
5715) for the augmented vs. 17643 (SD 5483) for the non-augmented
group (Figure 6). This differencewas statistically significant (
p
= 0.011).
Furthermore, the mode of failure changed significantly from cut-out in
the non-augmented group to implant failure (plate and/or screw
breakage) in the augmented specimens (Figure 6).
In summary of the above-presented studies [11,64,65] cement
augmentation of an angular stable locking plate shows beneficial
mechanical characteristics in osteoporoticdistal femur fracture fixation.
This method can enhance bone-implant anchorage significantly and
therefore has the potential to increase stability and avoid complications
(e.g. secondary loss of reduction, mal-union, non-union, cut-out). This
treatment option is not only possible for osteoporotic fractures, but also
for the treatment of periprosthetic distal femur fractures with a well-
fixed prosthesis and the possibility for fracture fixation. The additive
augmentation is a further option for surgeons to enhance stability and
reduce complications in osteoporotic
–
and only osteoporotic
–
distal
femur fractures. In our opinion it is a meaningful salvage procedure for
particular patients with severe osteoporotic/periprosthetic fractures.
Conclusion
Periprosthetic fractures continue to be a hot topic and to generate a
lot of interest in the field of trauma surgery. Several options exist in
periprosthetic fracture fixation: Cerclages are ideally suited to fix
radially displaced fragments around an intramedullary implant,
but they are susceptible to axial load and torsion. Due to the bony
surface geometry, cerclages provide a point-contact fixation and do not
compromise periosteal blood supply. Bicortical locking screw fixation
is effective but difficult on the level of the prosthesis stem. Inserted in
the embracement configuration around the intramedullary implant,
bicortical locking screws provide stable fixation in all load directions.
Double plating is another method to enhance construct stability.
Intramedullary implants increase fracture risk. The combination of
a retrograde nail and a hip endoprosthesis doubles the fracture risk
compared to a non-instrumented femur, whereas the combination of
two cemented well-fixed arthroplasty stems does not. Extramedullary
implants seem favorable for distal periprosthetic fracture fixation.
Concerning stability of the interprosthetic region, cortical thickness
of the femoral shaft is the more contributing factor compared to
interprosthetic distance.
Cement augmentation enhances angular-stable screw purchase in
the osteoporotic periprosthetic distal femur. Especially, if plate fixation
of an osteoporotic periprosthetic distal femur fracturewith awell-fixed
femoral component is considered, cement augmentation of the locking
screws increases construct stability and reduces failure rate.
Conflict of interest
The authors have no conflicts of interest.
References
[1]
Lindahl H, Malchau H, Herberts P, Garellick G. Periprosthetic femoral fractures
classification and demographics of 1049 periprosthetic femoral fractures from the
Swedish National Hip Arthroplasty Register. J Arthroplasty 2005;20:857
–
65.
[2]
Lindahl H, Malchau H, Oden A, Garellick G. Risk factors for failure after treatment of a
periprosthetic fracture of the femur. J Bone Joint Surg Br 2006;88:26
–
30.
[3]
Demos HA, Briones MS, White PH, Hogan KA, Barfield WR. A biomechanical comparison
of periprosthetic femoral fracture fixation in normal and osteoporotic cadaveric bone.
J Arthroplasty 2012;27:783
–
8.
[4]
Konstantinidis L, Hauschild O, Beckmann NA, Hirschmuller A, Sudkamp NP, Helwig P.
Treatment of periprosthetic femoral fractures with two different minimal invasive
angle-stable plates: Biomechanical comparison studies on cadaveric bones. Injury
2010;41:1256
–
61.
[5]
Lenz M, Perren SM, Gueorguiev B, Richards RG, Hofmann GO, Fernandez dell
’
Oca A, et al.
A biomechanical study on proximal plate fixation techniques in periprosthetic femur
fractures. Injury 2014;45(Suppl 1):S71
–
5.
[6]
Wähnert D, Schröder R, Schulze M, Westerhoff P, Raschke M, Stange R. Biomechanical
comparison of two angular stable plate constructions for periprosthetic femur fracture
fixation. Int Orthop 2014;38:47
–
53.
[7]
Lehmann W, Rupprecht M, Nuechtern J, Melzner D, Sellenschloh K, Kolb J, et al. What is
the risk of stress risers for interprosthetic fractures of the femur? A biomechanical
analysis. Int Orthop 2012;36:2441
–
6.
[8]
Moloney GB, Westrick ER, Siska PA, Tarkin IS. Treatment of periprosthetic femur fractures
around a well-fixed hip arthroplasty implant: span the whole bone. Arch Orthop Trauma
Surg 2014;134:9
–
14.
[9]
Lehmann W, Rupprecht M, Hellmers N, Sellenschloh K, Briem D, Puschel K, et al.
Biomechanical evaluation of peri- and interprosthetic fractures of the femur. J Trauma
2010;68:1459
–
63.
[10]
Forster MC, Komarsamy B, Davison JN. Distal femoral fractures: a review of fixation
methods. Injury 2006;37:97
–
108.
[11]
Wähnert D, Lange JH, Schulze M, Lenschow S, Stange R, Raschke MJ. The potential of
implant augmentation in the treatment of osteoporotic distal femur fractures: a
biomechanical study. Injury 2013;44:808
–
12.
[12]
Choi JK, Gardner TR, Yoon E, Morrison TA, Macaulay WB, Geller JA. The effect of fixation
technique on the stiffness of comminuted Vancouver B1 periprosthetic femur fractures.
J Arthroplasty 2010;25:124
–
8.
[13]
Moazen M, Mak JH, Etchels LW, Jin Z, Wilcox RK, Jones AC, et al. Periprosthetic femoral
fracture
–
a biomechanical comparison between Vancouver type B1 and B2 fixation
methods. J Arthroplasty 2014;29:495
–
500.
[14]
Lenz M, Perren SM, Gueorguiev B, Hontzsch D, Windolf M. Mechanical behavior of
fixation components for periprosthetic fracture surgery. Clin Biomech (Bristol, Avon)
2013;28:988
–
93.
[15]
Perren SM, Fernandez Dell
’
Oca A, Lenz M, Windolf M. Cerclage, evolution and potential
of a Cinderella technology. An overview with reference to periprosthetic fractures. Acta
Chir Orthop Traumatol Cech 2011;78:190
–
9.
[16]
Lenz M, Perren SM, Gueorguiev B, Richards RG, Krause F, Fernandez Dell
’
Oca A, et al.
Underneath the cerclage: an ex vivo studyon the cerclage-bone interface mechanics. Arch
Orthop Trauma Surg 2012;132:1467
–
72.
Fig. 6.
Number of cycles to failure (4> varus displacement) for the augmented and
non-augmented specimens, including the modes of failure: non-augmented speci-
mens failed by cut-out (upper right corner) and augmented failed by plate and/or
screw breakage (lower left corner).
M. Lenz et al. / Injury, Int. J. Care Injured 47S2 (2016) S44
–
S50
S49