

















 52 / 72
52 / 72

Up to now, it remains controversial, if screws could be anchored in
the cement mantle of cemented stems without damage of its integrity
provoking loosening of the stem [28]. The potential of this option has
not been investigated in detail jet. In osteoporotic bone, a screw
placement in the cement mantle would enhance screw purchase [28].
According to the actual consensus, a stem replacement is con-
sidered the best treatment option in case of stem loosening (Vancouver
type B2 fractures). In case of modest bone stock (Vancouver type B3),
treatment might end up at megaprostheses, whose surgery is very
consuming for the patient. In this context, screw fixation in the
prosthesis stemmight be an ideaworth considering [29]. Although this
technique is not yet established, prototype tests show promising
results, rendering the fixation independent of the surrounding bone
and allowing a minimal invasive surgery. Drilling the metal stem
requires special drill bits and a suction and collection system to remove
the metal debris, which would induce stem loosening, if kept in situ.
Future stem designs could provide holes for intraprosthetic screw
connection to avoid the drilling procedure.
Osteosyntheses of Vancouver type
A
G
fractures (fractures of the
greater trochanter) exhibit a high failure rate [30]. Current fixation
techniques include cerclages, tension band wiring and plates, but often
provide unidirectional stability in the laterosuperior direction. Most of
the biomechanical studies support this misunderstanding by focusing
on a one-dimensional load application. Tension forces of the gluteus
sling muscles acting on the greater trochanter are multidirectional,
especially in activities like stair climbing and rising from a chair [31].
Recent clinical and biomechanical data revealed that double plating on
the anterior and lateral aspect of the greater trochanter improves
fixation strength and lowers failure rates [32,33].
How do implants affect bone strength?
The number of orthopedic implants continuously rises, especially
in the hip and knee, which impacts the stability of the affected bones.
Considering a scenario with a single proximal prosthesis in the
femur, changes in the stiffness of the bone increases the risk for a
fracture of the femur of up to 30% [9,34]. If, at the same time, another
intramedullary force carrier (i.e. a nail) is implanted on the ipsilateral
side next to a proximal prosthesis the risk for interprosthetic fracture
further increases (Figure 3). Compared to an unoperated native femur
only half the force is required to induce a fracture to the operated femur
[9]. Thus, this combination represents one of the highest risk for a
fracture. It is somewhat different when two cemented stems from a hip
and knee prosthesis come to lie in the femur. Own biomechanical
studies have shown that in this scenario, the risk for a fracture is
different. This may be due to the locking screws of the nail, which
represent a
“
locus of minor resistance
”
because of their transmitted
stress riser to the cortex. The distance between these cemented
implants does not seem to play an important role. Much more
important is the cortical thickness of the femur that has major
influence on fracture risk [35]. The risk of suffering from a fracture
between a proximal prosthesis and an extramedullary implant for
example a locking plate is significantly lower. It can be concluded that
an extramedullary plate might be biomechanically advantageous for
the treatment of supracondylar femoral fractures in the presence of a
hip prosthesis at the proximal side.
There is abundant clinical evidence that loosened prostheses, either
cemented or uncemented increases the risk for a fracture around the
prostheses [36]. However, this scenario is difficult to simulate in
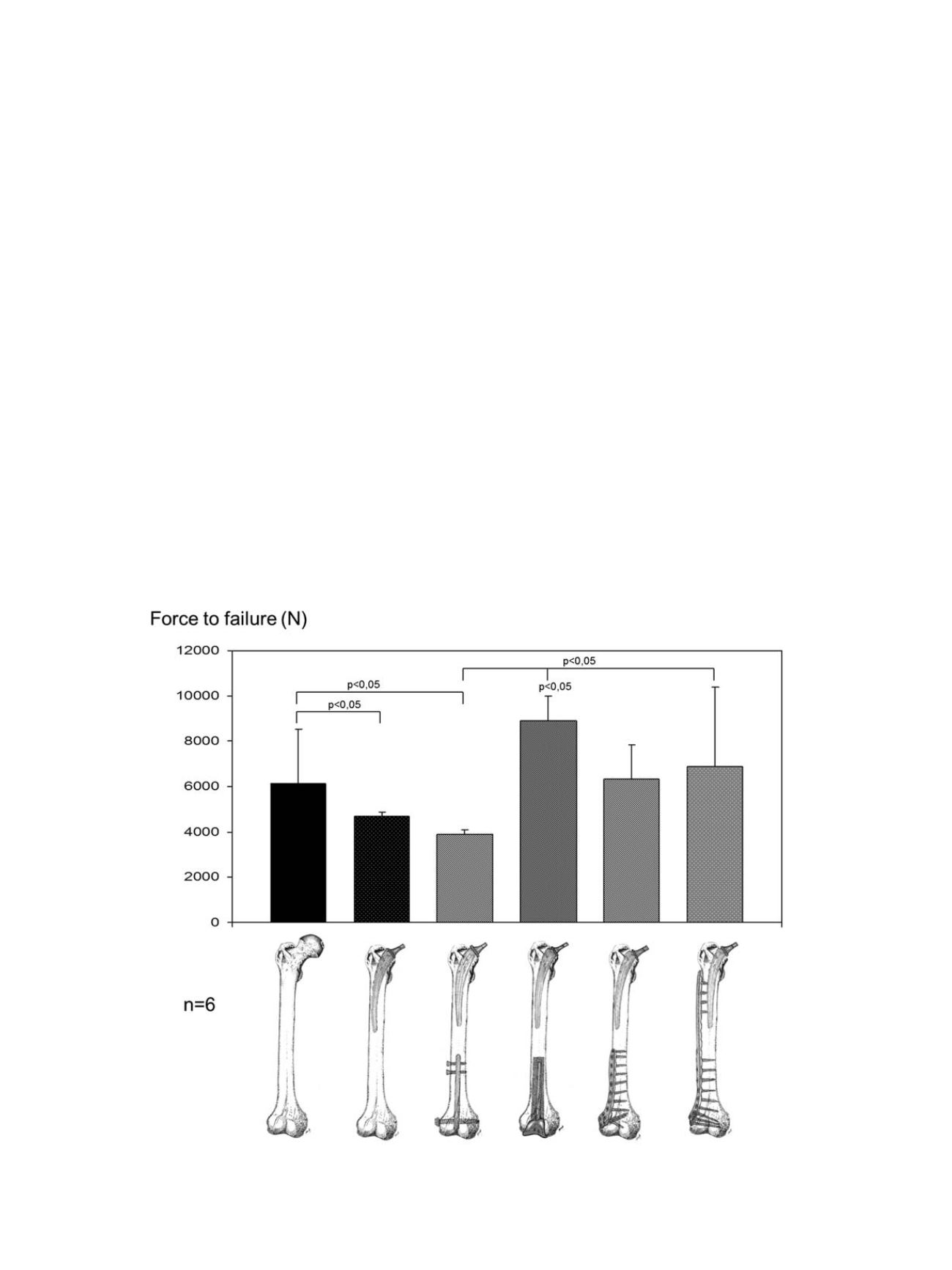
Fig. 3.
Fracture strength. Average load to failure in different groups in a biomechanical testing. The required fracture force further decreases considerably if a retrograde nail was
implanted. A constrained knee prosthesis did not show this effect; the large cement mantle imparts a very high required fracture force. With extramedullary locking stable
plates in the distal femur, the risk for a fracture is not as high as with a retrograde nail.
M. Lenz et al. / Injury, Int. J. Care Injured 47S2 (2016) S44
–
S50
S46