

















 21 / 72
21 / 72

the distribution of bone mineral was shown to be dependent on
anatomical location within the proximal femur, with a higher
variability of mineralization between the greater and lesser trochanter
regions of ovariectomized sheep (Figure 5), which coincides with the
intertrochanteric fracture line [66]. These findings were undetectable
by focusing solely on bone mineral density and are corroborated by
studies of human osteoporotic trabeculae [64,67].
Rapid increases in bone resorption by osteoclasts occur at the
onset of osteoporosis but abate over time. As such the disparity
between different studies might also relate to the extent of disease
progression, the timing of which likely varies between animal models
and human bone. A recent study sought to understand how trabecular
tissue mineralization is altered over prolonged estrogen depletion and
compared this to normal age-related changes in trabecular bone tissue
composition [68]. Bone mineral density distribution parameters were
compared in trabeculae from the proximal femora of ovariectomized
sheep that underwent estrogen deficiency for 12 or 31 months and
age-matched controls. It was reported that normal ageing increases
mean mineralization and mineral heterogeneity at a trabecular level
and that these differences arise due to an increase in the mineralisa-
tion of the deep lamellae of the trabeculae with ageing (Figure 6).
However, prolonged estrogen deficiency (31 months) leads to signi-
ficantly decreased mean mineralization compared to trabeculae from
both aged matched controls and a shorter duration of estrogen
deficiency (12 months) (compare with Figure 5). Increased rates of
bone turnover during estrogen deficiency could explain this lower
meanmineralization. However, reductions inmineralizationwere non-
uniform within the proximal femur [68]. The underlying mechanisms
by which trabecular mineral heterogeneity is altered during osteo-
porosis might be due to hypermineralized osteocyte lacunae in
osteoporotic trabecular bone and an increased bone turnover [69].
Additionally, this variability might be related to local variations in the
mechanical environment, which might lead to alterations in tissue
mineral content at those regions regulated by mechanosensitive bone
cells [69]. Together these recent studies [66,68] reveal the importance
of duration and anatomical location in assessing the effects of estrogen
deficiency on trabecular bone mineralization and may explain
discrepancies regarding the effect of estrogen deficiency between
previous studies.
In summary, it is becoming increasingly clear that, even though
overall trabecular bone mass and strength are reduced during osteo-
porosis, the scarce trabecular tissue that remains is more hetero-
geneous, with regions of trabecular tissue that are more mineralized,
stiffer and stronger. It would also appear that these changes are a
transient and site-specific characteristic of osteoporosis, whereby the
trabecular tissue properties are altered varyingly as the disease
progresses.
Changes in cortical bone with aging and osteoporosis
The biomechanical competence of a bone is determined by the
amount and quality of bone material and evenmore importantly by the
arrangement of the material in space. Geometrical measures including
bone size, cross-sectional area or area moment of inertia explain up to
80% of the biomechanical competence of whole bones. For the distal
radius, the best predictors of fracture load were measures of cortical
bone mass, cortical area and cortical width [70]. For the proximal
femur cortical area, size of the femoral neck and area moment of inertia
were the strongest predictors of fracture load [70]. The combination
of individual parameters in multiple regression models has provided
further evidence that geometrical measurements considerably
improve the prediction of bone strength beyond measurement of
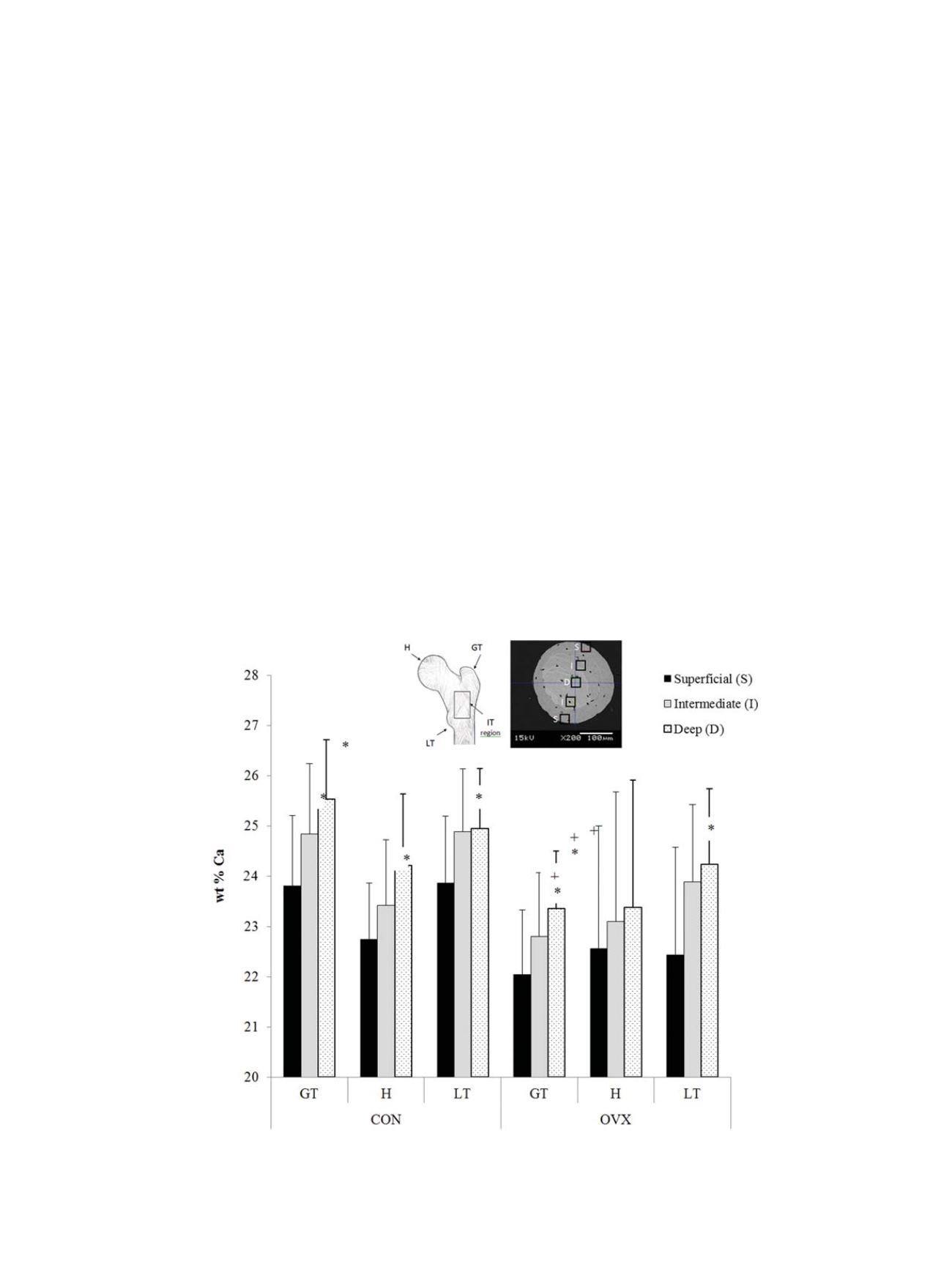
Fig. 6. Trabecular mineralization in prolonged estrogen deficiency
Spatial distribution of calcium (wt% Ca) between superficial, intermediate, and deep lamellae in the
greater trochanter (GT), head (H) and lesser trochanter (LT) regions of the proximal femur from 31 month ovariectomized sheep (OVX) and aged matched controls (CON). * indi-
cates significantly different to deep lamellae within the same femoral region of the indicated group. + indicates significant difference to the same ROI of the CON group. Data
from [65].
G. Osterhoff et al. / Injury, Int. J. Care Injured 47S2 (2016) S11
–
S20
S15